Section
Author
Last edited
Sep 11, 2024 4:53 PM
Dot phrases
⚠️ Close follow-up
Frequency of GFR and albuminuria monitoring (consider increased frequency depending on rate/degree of change). Early CKD (q1 year), GFR 30-45 (q6 mo), GFR 20-30 (q3 mo), GFR < 20 (co-manage with nephrology)
📬 Referral to specialist
Acutely worsening CKD or patients with GFR < 20 who you think might need dialysis or a kidney transplant down the road
🚨 Send to the ED
Definition
- CKD = GFR < 60 or kidney damage (proteinuria, hematuria, imaging abnormal, electrolyte abnormality 2/2 to renal) for > 3 months
Diagnosis and workup
- Lab studies: CBC, CMP, lipid panel, uric acid
- Urine studies: UA with microscopy, urine sediment exam, spot UProt/Cr, CBC (for CKD-related anemia)
- Renal US: in CKD usually shows echogenic, small kidneys bilaterally (some exceptions are DM, myeloma, HIV, amyloid, PCKD).
- If age >50 with proteinuria or anemia, consider SPEP/UPEP/IFE (or serum free light chains instead of SPEP/UPEP/IFE)
Classification
Classification should focus on AGC: (1) Albuminuria, (2) GFR, (3) Cause
GFR Category | GFR (ml/min/1.73m2) | Terms |
G1 | >90 | Normal or high |
G2 | 60-89 | Mild |
G3a | 45-59 | Mild to moderate |
G3b | 30-44 | Moderate to severe |
G4 | 15-29 | Severe |
G5 | <15 | End stage |

ACR (albumin:Cr ratio) Category | Mg albumin / g creatinine | Terms |
A1 | <30 | Normal to mild |
A2 | 30-300 | Moderate |
A3 | >300 | Severe |
Management
Prevention of CKD progression
- Avoid nephrotoxic agents such as NSAIDs, PPIs, contrast studies, aminoglycosides, acyclovir, phosphate-based bowel prep, and baclofen
- Renally dose medications, including antimicrobials, atenolol, colchicine, DOACs, diabetes medications, gabapentin, levetiracetam, metoclopramide, and opioids
- Encourage regular exercise and smoking cessation.
- Treat underlying hepatitis C virus (HCV) infection.
Management of co-morbidities
- Blood pressure:
- Treat BP to goal < 130/80 (AHA 2017) or <120 SBP (KDIGO 2021)
- In resistant hypertension with HFrEF, consider spironolactone
- Proteinuria:
- For patients with A2 albuminuria (UACR >300 mg/d) → start ACEi/ARBs with the goal of reducing UACR to <300 mg/d.
- SGLT2 inhibitors are recommended if GFR >20 mL/min/1.73 m², as they have been shown to slow CKD progressionExpect a slight decline in GFR here too, this is acceptable
- Diabetes:
- Aim for an HbA1c <7%;
- Continue metformin if GFR >45
- Start SGLT2 inhibitors if GFR >20
- GLP-1 receptor agonists if GFR >30
- Insulin is safe at any GFR
- ASCVD:
- Prescribe statin therapy for patients aged 50 years or older or if ASCVD risk is 10% or greater
An rise in Cr 20-30% can be expected when starting ACEi/ARBs. Recheck labs within 1 week to confirm that the Cr does not continue to increase
Lifestyle and nutrition
- For CKD stages G3-G5 with serum phosphate >5.5 mg/dL, dietary phosphate should be restricted to 0.55-0.60 g/kg/day.
- In CKD stages G4-G5, advise patients to avoid high-potassium foods.
- Refer to a renal dietitian for personalized nutrition planning.
- For patients with nephrotic syndrome and CKD stages G3-G5, protein supplementation should be 0.6-0.8 g/kg/day
- Prescribe vitamin B complex (Nephrovite, Nephrocaps, Triphrocaps) to provide essential vitamins
- If edema is present, recommend fluid restriction and a sodium intake of less than 2 g/day.
Management of CKD complications
- Metabolic acidosis: Prescribe sodium bicarbonate 650-1300 mg TID (or 0.5 meq/kg/day) to maintain serum bicarbonate >22 mmol/L.
- Anemia: Dx of exclusion. Check Hgb q3 months if anemic, not on HD and not on erythropoiesis-stimulating agents (ESAs). ESAs if Hb <10 with a target Hgb of 10-11.5 g/dL. Reasonable to trial PO iron if %sat <30 and ferritin < 500 and anemic.
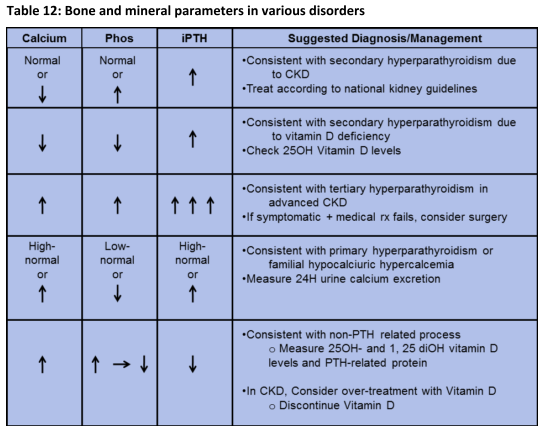
- Bone mineral Disease (BMD): treat to iPTH goal < 9x ULN
- Rx: Phosphate binder and ergocalciferol (goal 30)
- Hold Vit D if corr Ca > 10.2 or phos > 4.6
- Up to Stage IV: iPTH goal ULN
- iPTH goal
- Measure Ca, Phos q3 months
- Initiate phosphate binders such as sevelamer 800 mg TID with meals to maintain serum phosphate <5.5 mg/dL
- Hyperkalemia: Use loop diuretics or potassium binders like sodium zirconium cyclosilicate (Lokelma) as needed.
- Edema: Manage with diuretics as needed or on a standing basis.
Other considerations
- In stage 4-5 CKD, avoid venipuncture, IV placement, PICC lines, and subclavian catheters in arm most suitable for future vascular access (usually non-dominant arm)
- Pneumococcal vaccine (both PPS-23 and PCV-13) should be administered once, at least one year apart, and yearly flu vaccine. Hepatitis B vaccination if progressing to dialysis and/or transplantation.
Indications for referral to nephrology
- CKD Stage G3b
- Gradual progression: >25% decline in GFR or >5/yr annual decline
- AKI or sudden sustained drop in GFR
- Proteinuria > 300 mg/day or equivalent
- Unexplained persistent hematuria >20 / hpf or RBC casts
- Refractory HTN on 4 agents with CKD
- Persistent electrolyte abnormalities
- Recurrent nephrolithiasis
- Hereditary kidney disease
On this page
- Definition
- Diagnosis and workup
- Classification
- Management
- Prevention of CKD progression
- Management of co-morbidities
- Lifestyle and nutrition
- Management of CKD complications
- Other considerations
- Indications for referral to nephrology
Resources
‣
Website: NavigationOutpatient Guide